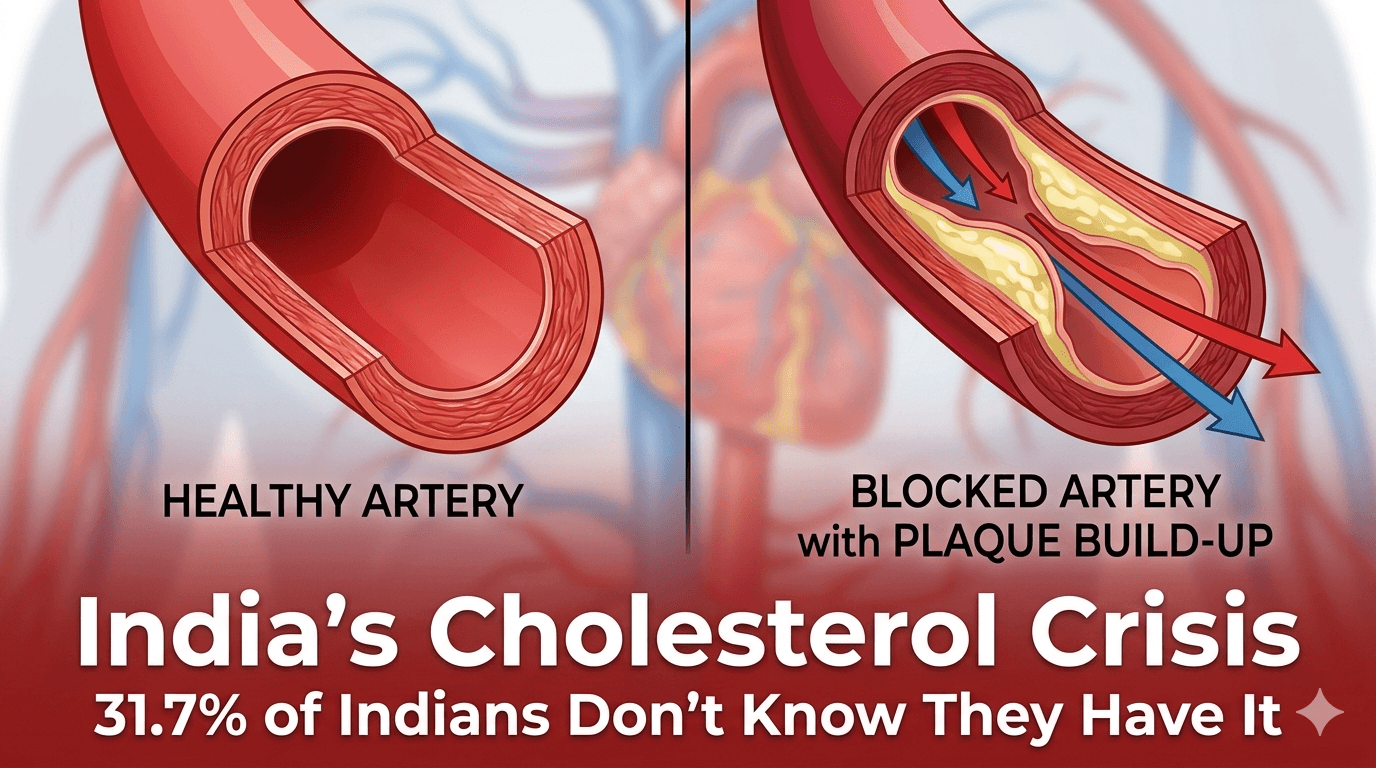
India's Silent Cholesterol Crisis — Why 31.7% of Indians Have Abnormal Cholesterol and Don't Know It
There is a health crisis unfolding in India that has no symptoms, no pain and no warning — until the day it causes a heart attack or stroke.
A major 2026 report analysing four lakh health check-ups found that 31.7% of Indians have abnormal cholesterol levels, creating elevated cardiovascular risk that is particularly concerning for the Indian workforce. (Source: Prompt Personnel)
Nearly one in three Indians. Walking around feeling completely healthy. With no idea that their blood vessels are being slowly, silently damaged.
Over 33% of Indians exhibit early warning signs of chronic diseases — often appearing healthy but possessing markers for heart disease, obesity or diabetes — leading experts to call this a silent lifestyle disease crisis.
Cholesterol is the perfect example of this silent crisis. It causes no symptoms. It produces no pain. It gives no warning. And then one day, after years of silent damage to arterial walls — it causes the heart attack or stroke that kills or permanently disables.
As someone from the pharmaceutical field, cholesterol management is something I feel strongly about — because the gap between what most Indians understand about cholesterol and what the science actually says is enormous and dangerous.
This blog will close that gap.
What Is Cholesterol — Really?
Cholesterol has been so thoroughly demonised in popular health culture that most people don't realise it is an essential molecule — not a toxin.
Cholesterol is a waxy, fat-like substance produced primarily by your liver (about 75-80% of total cholesterol) with the remainder coming from dietary sources. It is a structural component of every cell membrane in your body, is essential for the production of steroid hormones including oestrogen, testosterone and cortisol, is required for the synthesis of Vitamin D from sunlight, and is a precursor for bile acids that are essential for fat digestion.
Without cholesterol, you cannot survive.
The problem is not cholesterol itself — it is when specific cholesterol fractions accumulate in excess in the wrong places — particularly the walls of arteries — causing the inflammation and structural damage that leads to cardiovascular disease.
Understanding cholesterol transport — the key to understanding the numbers:
Cholesterol does not travel freely in the bloodstream. Being fat-based, it cannot dissolve in blood (which is water-based). Instead it is packaged into protein-lipid particles called lipoproteins that act as transport vehicles.
The primary lipoproteins relevant to cardiovascular health are:
- LDL (Low-Density Lipoprotein): Transports cholesterol from the liver to tissues throughout the body. When LDL levels are excessive, LDL particles penetrate arterial walls, become oxidised and trigger the inflammatory cascade that forms arterial plaques — the underlying cause of most heart attacks and strokes. This is why LDL is colloquially called "bad cholesterol" — though the reality is more nuanced. It is not bad in normal amounts and performing its normal function — it is dangerous in excess, particularly when oxidised.
- HDL (High-Density Lipoprotein): Transports cholesterol from peripheral tissues back to the liver for processing and excretion — a process called reverse cholesterol transport. Higher HDL is associated with lower cardiovascular risk. This is why HDL is called "good cholesterol."
- VLDL (Very Low-Density Lipoprotein): Produced by the liver to transport triglycerides (blood fats) to tissues. Elevated VLDL drives elevated triglycerides — an independent cardiovascular risk factor.
- Triglycerides: Not technically cholesterol but measured in the lipid panel. Elevated triglycerides — driven primarily by excess refined carbohydrates, sugar and alcohol — independently increase cardiovascular risk and are particularly problematic for Indians.
Understanding Your Lipid Numbers — What They Actually Mean
Most Indians who have had a lipid profile test look at the results, see them marked "normal" or "abnormal" and have little idea what the numbers actually mean or what drives them. Let me explain each clearly.
Total Cholesterol
Total cholesterol is the sum of LDL + HDL + VLDL cholesterol. It is the least useful number in the lipid panel — because high total cholesterol driven by high HDL (a good thing) looks the same as high total cholesterol driven by high LDL (a bad thing).
However as a broad screening indicator:
- Below 200 mg/dL — desirable
- 200-239 mg/dL — borderline high
- 240 mg/dL and above — high
LDL Cholesterol — The Number That Matters Most
LDL is the primary therapeutic target in cardiovascular risk management. Target levels depend on your overall cardiovascular risk:
- Low risk (no major risk factors): Below 130 mg/dL
- Moderate risk: Below 100 mg/dL
- High risk (diabetes, established heart disease, multiple risk factors): Below 70 mg/dL
- Very high risk (recent heart attack, stroke): Below 55 mg/dL
HDL Cholesterol — Higher Is Better
- Below 40 mg/dL in men, below 50 mg/dL in women — low HDL, increased risk
- 40-60 mg/dL — acceptable
- Above 60 mg/dL — protective, associated with lower cardiovascular risk
Triglycerides — The Hidden Indian Problem
- Below 150 mg/dL — normal
- 150-199 mg/dL — borderline high
- 200-499 mg/dL — high
- 500 mg/dL and above — very high, risk of pancreatitis
Why Indians Are Uniquely Vulnerable
India's cholesterol crisis is not simply explained by diet and lifestyle — though these are important. Indians have specific genetic and physiological characteristics that make them particularly susceptible to cardiovascular disease from cholesterol abnormalities.
South Asian cardiovascular paradox
Indians develop cardiovascular disease approximately 10 years earlier than Western populations. Heart attacks occur at younger ages, at lower body weights and at lower LDL levels than would be expected from Western risk models. An Indian with the same lipid profile as a European has significantly higher cardiovascular risk.
genetic predisposition to atherogenic dyslipidaemia
Indians genetically tend toward high triglycerides, low HDL and high Lipoprotein(a) — a genetic variant of LDL that is highly atherogenic and not reduced by standard lifestyle interventions. Lipoprotein(a) — often abbreviated Lp(a) — is elevated in approximately 25-30% of Indians and is an independent, underappreciated cardiovascular risk factor.
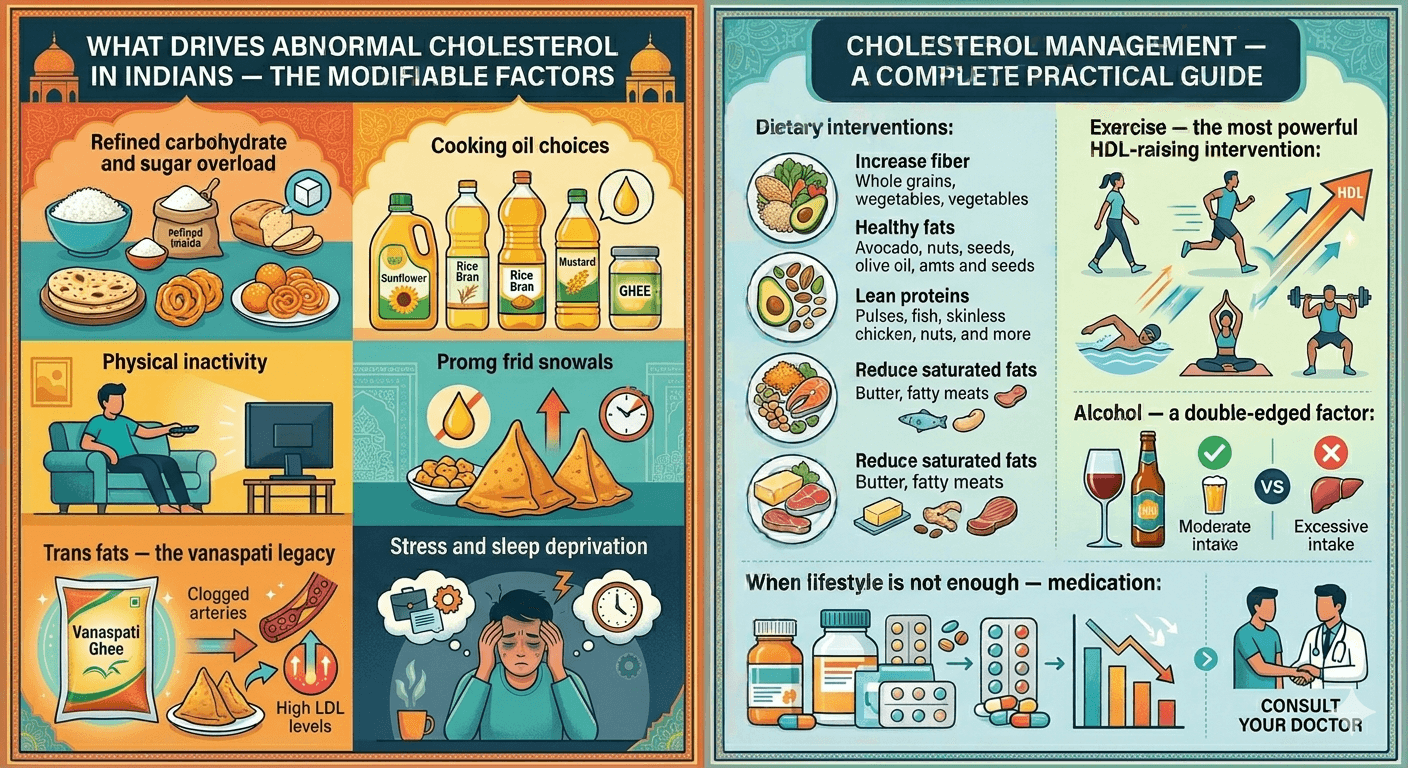
Cholesterol Management — A Complete Practical Guide
Dietary interventions with strong evidence:
- Increase soluble fiber: Soluble fiber — found in oats, barley, legumes (dal, rajma, chana), fruits (apple, pear, amla) and psyllium husk (isabgol) — binds bile acids in the gut and prevents their reabsorption. The liver must then use cholesterol to produce new bile acids — directly reducing circulating LDL.
- Reduce refined carbohydrates aggressively: For elevated triglycerides — the primary Indian lipid problem — reducing refined carbohydrates (white rice, maida, sugar, packaged snacks, sweetened beverages) is more effective than reducing dietary fat.
- Increase omega-3 fatty acids: Omega-3s — from walnuts, flaxseeds, chia seeds and for non-vegetarians from fatty fish — significantly reduce triglycerides.
- Nuts — particularly walnuts and almonds: Multiple clinical trials have demonstrated that regular nut consumption reduces LDL, raises HDL and reduces cardiovascular events.
Exercise — the most powerful HDL-raising intervention:
150-180 minutes of moderate-intensity aerobic exercise weekly — brisk walking, cycling, swimming — raises HDL by 5-10%, reduces triglycerides by 15-20% and improves LDL quality. Even moderate exercise produces meaningful lipid benefits within 4-8 weeks.
What Tests to Get and When
Fasting lipid profile: The standard test — measures total cholesterol, LDL, HDL, VLDL and triglycerides after 9-12 hours of fasting.
Who should test: All Indians above 20 years should have a fasting lipid profile at least every 5 years. Above 40 years or with any risk factor (family history, diabetes, hypertension, obesity, smoking) — annually.
Conclusion
Know your numbers. Know your risk. And if your doctor recommends treatment — take it.
The 31.7% of Indians with abnormal cholesterol who don't know they have it will not remain asymptomatic forever. Don't let a preventable heart attack be your first symptom.
🛒 Recommended Product
Omega-3 supplementation is one of the most evidence-based ways to reduce triglycerides — one of the most common lipid problems in Indians. This fish oil supplement provides EPA and DHA at clinically relevant doses. Always take with food for best absorption and to minimise any fishy aftertaste.
View MuscleBlaze Omega-3 on Amazon →References
- Joshi SR, et al. Prevalence of dyslipidaemia in urban and rural India. J Assoc Physicians India. 2014;62(2):26-35.
- Gupta R, et al. Lipid abnormalities and coronary heart disease in India. J Assoc Physicians India. 2008;56:257-264.
- Stone NJ, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol. J Am Coll Cardiol. 2014;63(25 Pt B):2889-934.
Written by — Dharmil Pandya
Medical Writer | Founder, Healthier Tomorrow
#HeartHealthIndia #CholesterolCrisis #PreventiveCare #LipidProfile #IndianWellness