Endometriosis in Indian Women — The Disease That Takes 7-10 Years to Diagnose
Every month, millions of Indian women experience pain so severe during their periods that they cannot go to work, school or function normally. They take painkillers, apply heat, rest in bed and wait for it to pass. They tell their doctors. They are told — by family, by society, and far too often by medical professionals — that period pain is normal. That they should tolerate it. That all women go through this.
They are being failed by a profound gap in medical awareness and cultural understanding.
For a significant proportion of these women, their pain is not normal menstruation. It is endometriosis — a chronic, systemic disease that in many cases is destroying their fertility, damaging their organs and severely impairing their quality of life, while going undiagnosed for an average of 7-10 years.
Endometriosis is not rare. It is not a Western condition. It is not caused by not getting pregnant early or working too hard. And it is most certainly not psychological.
It is one of the most common chronic diseases affecting Indian women — and one of the most inadequately addressed.
This blog exists to change that, one informed reader at a time.
What Is Endometriosis?
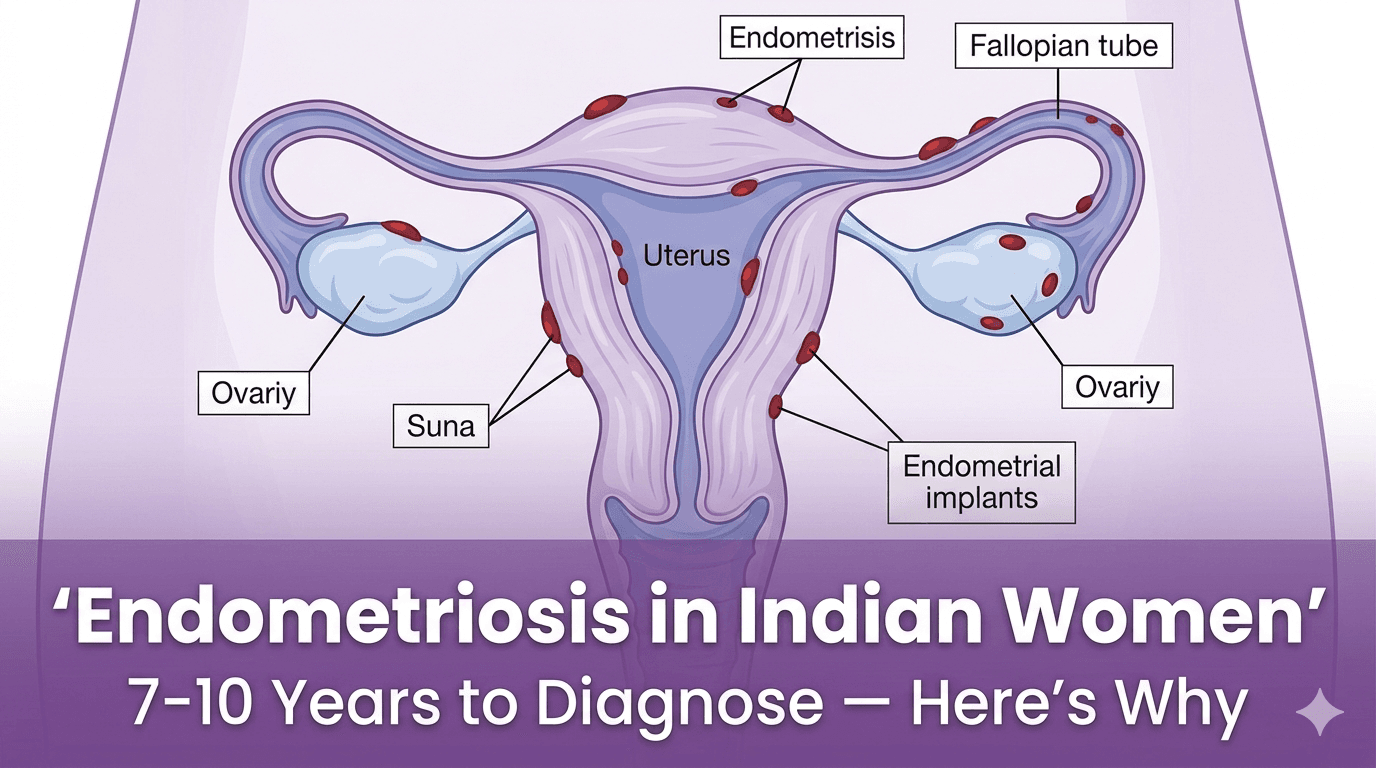
Endometriosis is a chronic inflammatory condition in which tissue similar to the endometrium — the lining of the uterus — grows outside the uterus in locations where it does not belong.
This misplaced tissue — called endometrial implants or lesions — can be found on or in:
- The ovaries — forming fluid-filled cysts called endometriomas or "chocolate cysts"
- The fallopian tubes
- The outer surface of the uterus
- The bowel and rectum
- The bladder
- The peritoneum — the membrane lining the abdominal cavity
- In severe cases — the diaphragm, lungs and even the brain
Like the normal endometrium, this misplaced tissue responds to the hormonal cycle — thickening during the first half of the cycle and attempting to shed during menstruation. But unlike the normal endometrium, it has nowhere to go. The blood and tissue cannot exit the body. Instead it irritates surrounding tissues, causes inflammation and, over time, forms adhesions — bands of scar tissue that can bind organs together — and fibrosis.
The result is a progressive, inflammatory disease that, if untreated, can cause:
- Chronic pelvic pain — not just during periods but throughout the cycle
- Severe, debilitating menstrual pain (dysmenorrhoea)
- Pain during or after sexual intercourse (dyspareunia)
- Pain during bowel movements or urination — particularly during menstruation
- Heavy or irregular periods
- Fatigue — often profound and underappreciated
- Infertility — endometriosis is found in 30-50% of women with fertility difficulties
- Bowel and bladder symptoms — bloating, constipation, diarrhoea, urinary frequency
How Common Is Endometriosis in India?
Endometriosis affects approximately 10% of women of reproductive age globally. In India — with a female reproductive age population of over 400 million — this translates to approximately 42 million women living with endometriosis.
To put this in perspective: endometriosis is more common in India than diabetes is in many countries. It affects more Indian women than breast cancer, cervical cancer and ovarian cancer combined.
Yet most Indians — including many doctors — have never had a conversation about it.
The diagnosis gap is staggering. Studies suggest that globally, and particularly in India, the average time from symptom onset to diagnosis is 7-10 years. Many Indian women are diagnosed only when they present with infertility — having lived with the disease and its consequences for a decade without understanding what was causing their suffering.
Why Does It Take So Long to Diagnose?
The diagnostic delay in endometriosis — in India and globally — is driven by a convergence of medical, social and cultural factors that are important to understand.
"Period pain is normal" — the most dangerous myth in women's health
The normalisation of menstrual pain is the single most damaging barrier to endometriosis diagnosis globally. In Indian culture — where menstruation is often not discussed openly, where girls are taught that period discomfort is expected and where complaints are frequently dismissed with "every woman goes through this" — women with endometriosis rarely receive the validation they need to persist in seeking diagnosis.
The critical distinction that every Indian woman and every doctor must understand: normal menstrual discomfort is mild and manageable. Pain that requires prescription painkillers, causes vomiting, prevents normal activity or worsens over time is not normal and warrants investigation.
Medical knowledge gaps
Endometriosis is underrepresented in Indian medical education. Many general practitioners and even some gynaecologists have limited exposure to endometriosis during training. This means that women presenting with the classic symptoms are frequently diagnosed with irritable bowel syndrome, pelvic inflammatory disease, ovarian cysts or anxiety — each a legitimate diagnosis but not the underlying cause.
The diagnostic challenge
Endometriosis cannot be diagnosed through a blood test or a routine ultrasound. Standard pelvic ultrasound misses most endometriosis — it can detect ovarian endometriomas (chocolate cysts) but misses superficial peritoneal lesions and deep infiltrating endometriosis, which are the most common forms.
The gold standard for diagnosis is laparoscopy — a minimally invasive surgical procedure in which a camera is inserted into the abdomen to directly visualise endometrial implants. This procedural requirement — needing a surgeon willing to look for and recognise endometriosis during laparoscopy — creates a significant access and knowledge barrier in India.
The Four Stages of Endometriosis
Endometriosis is classified into four stages based on the extent and location of disease:
- Stage I (Minimal): Small, isolated implants on the peritoneum or ovaries. Minimal adhesions. Symptoms may be mild — or surprisingly severe.
- Stage II (Mild): More implants, slightly deeper. Small endometriomas may be present. More adhesions.
- Stage III (Moderate): Multiple deep implants. Endometriomas on one or both ovaries. Adhesions around the fallopian tubes and ovaries that may affect their function.
- Stage IV (Severe): Extensive deep implants. Large endometriomas. Significant adhesions that may cause the uterus, ovaries, fallopian tubes and bowel to become adherent to each other — a condition called a "frozen pelvis" in severe cases.
A critical point: Stage I endometriosis can cause excruciating pain. Stage IV can occasionally cause minimal symptoms. The surgical stage does not predict symptom severity. This is why "but your ultrasound was normal" is not a satisfying or appropriate dismissal of a woman's symptoms.

Endometriosis and Fertility
This is often the aspect of endometriosis that most concerns Indian women — given the cultural, familial and personal significance of fertility in Indian society.
Endometriosis is found in approximately 30-50% of women with infertility. It affects fertility through multiple mechanisms:
- Ovarian endometriomas damage ovarian tissue and reduce ovarian reserve — the number of eggs available
- Adhesions distort pelvic anatomy — kinking or blocking fallopian tubes, preventing the egg from reaching the uterus
- The inflammatory environment of the pelvis impairs egg quality, sperm function and embryo implantation
- In severe cases, anatomical distortion makes natural conception essentially impossible
The relationship between endometriosis and fertility is not absolute — many women with even Stage III or IV endometriosis conceive naturally. But the risk is real and the evidence for earlier diagnosis and treatment improving fertility outcomes is compelling.
Symptoms You Should Never Dismiss
Primary symptoms:
- Period pain that is severe enough to require strong painkillers, prevent normal activity or cause vomiting
- Period pain that is getting progressively worse over time rather than staying stable
- Pelvic pain that occurs outside of your period — mid-cycle, after ovulation or throughout the month
- Deep pain during sexual intercourse — felt internally rather than at the surface
- Pain or bleeding during bowel movements — particularly during menstruation
- Urinary urgency, frequency or pain — particularly cyclically worsening with menstruation
- Heavy periods with clots
Secondary symptoms — often overlooked:
- Profound fatigue — not just tiredness but the kind of exhaustion that doesn't improve with rest
- Bloating — sometimes described as "endo belly" — cyclical severe abdominal distension
- Shoulder tip pain during menstruation — a red flag for diaphragmatic endometriosis
- Cyclically worsening bowel symptoms — alternating constipation and diarrhoea during menstruation
- Recurrent miscarriage
Management — What Actually Helps
Medical management:
Hormonal therapy is the first-line medical treatment. It works by reducing or eliminating the hormonal fluctuations that drive endometriosis activity:
- Combined oral contraceptive pill — used continuously to suppress menstruation
- Progestins — including dienogest, which has the strongest evidence base specifically for endometriosis and is available in India
- GnRH agonists — including Lupride, create a temporary medical menopause, often used before surgery
- Levonorgestrel intrauterine device (Mirena) — highly effective for pain and heavy periods
Complementary approaches with evidence:
- Anti-inflammatory diet: Reducing red meat and refined carbohydrates; increasing omega-3s and fiber
- Turmeric (curcumin): Demonstrated anti-inflammatory effects relevant to endometriosis
- Regular moderate exercise: Reduces prostaglandin production and improves pain modulation
- Yoga and mindfulness: Evidence supports benefit for chronic pelvic pain
The Indian Context — Cultural Barriers
Discussing endometriosis in India requires acknowledging the specific cultural barriers that compound the medical ones:
- Menstrual taboo: Menstruation is often not discussed openly, leading to silent suffering
- Pain tolerance as virtue: Narratives framing women's pain tolerance as strength discourage seeking care
- Fertility pressure: Stigma surrounding infertility can prevent open discussion of endometriosis
- Family gatekeeping: Barriers to gynaecological care for young unmarried women
Conclusion
Your pain deserves investigation. Your symptoms deserve to be taken seriously. You are not being dramatic, weak or oversensitive.
Severe menstrual pain is not normal. Pain that interferes with your life is not something you must simply endure. And the 7-10 year diagnostic delay that millions of Indian women experience is not inevitable — it ends when women are informed enough to demand better.
If you recognise your experience in this blog — please seek specialist assessment. If your current doctor dismisses your concerns — find another. If you know a woman who is suffering — share this information with her.
Endometriosis is chronic, progressive if untreated, and eminently manageable with the right diagnosis and treatment. You deserve that care.
🛒 Recommended Product
Omega-3 fatty acids have clinical evidence for reducing the prostaglandin-driven inflammation and pain that characterises endometriosis. EPA and DHA at 2-3g daily — taken with food — is the evidence-supported dose for anti-inflammatory effects relevant to endometriosis pain management.
View Omega-3 Supplement on Amazon →References
- Zondervan KT, et al. Endometriosis. Nat Rev Dis Primers. 2018;4(1):9.
- Parasar P, et al. Endometriosis: epidemiology, diagnosis and clinical management. Curr Obstet Gynecol Rep. 2017;6(1):34-41.
- Singh N, et al. Endometriosis in India — challenges and unmet needs. J Obstet Gynaecol India. 2020;70(4):271-276.
Written by — Dharmil Pandya
Medical Writer | Founder, Healthier Tomorrow
#EndometriosisIndia #WomensHealth #PeriodPain #EndoWarrior #IndianWellness