Perimenopause in Indian Women — The 10 Years Before Menopause That Nobody Talks About
You are 38 years old. Your periods have become unpredictable — sometimes heavy, sometimes light, sometimes arriving two weeks early. You are exhausted despite sleeping 8 hours. Your moods shift in ways that feel foreign to you. You are gaining weight around your middle despite no change in diet. Your sleep is disrupted by what feel like sudden waves of warmth at night.
Your doctor runs blood tests. Everything comes back "normal." You are told it's stress.
But it's not stress. It's perimenopause.
And you are far from alone. Millions of Indian women are living through this transition right now — without a name for what they're experiencing, without information about what's happening in their bodies, and without support.
This blog exists to change that.
What Is Perimenopause?
Perimenopause literally means "around menopause." It is the transitional phase during which a woman's body gradually shifts from its reproductive years toward menopause — defined as 12 consecutive months without a period.
What most people don't realise is that this transition doesn't happen overnight. It is a gradual process that typically begins 8-10 years before menopause actually occurs — meaning it can start as early as the mid-30s for many women.
The average age of menopause in Indian women is 46-47 years — 4-5 years earlier than the global average of 51. This means Indian women may begin perimenopause as early as their mid-to-late 30s — during years when they are managing careers, raising children, caring for aging parents and navigating peak life responsibilities.
This timing makes the Indian perimenopause experience uniquely challenging — and uniquely underaddressed.
What's Actually Happening in Your Body
Understanding the biology makes the experience less frightening and more manageable. As a pharma professional, let me explain what is happening hormonally during perimenopause.
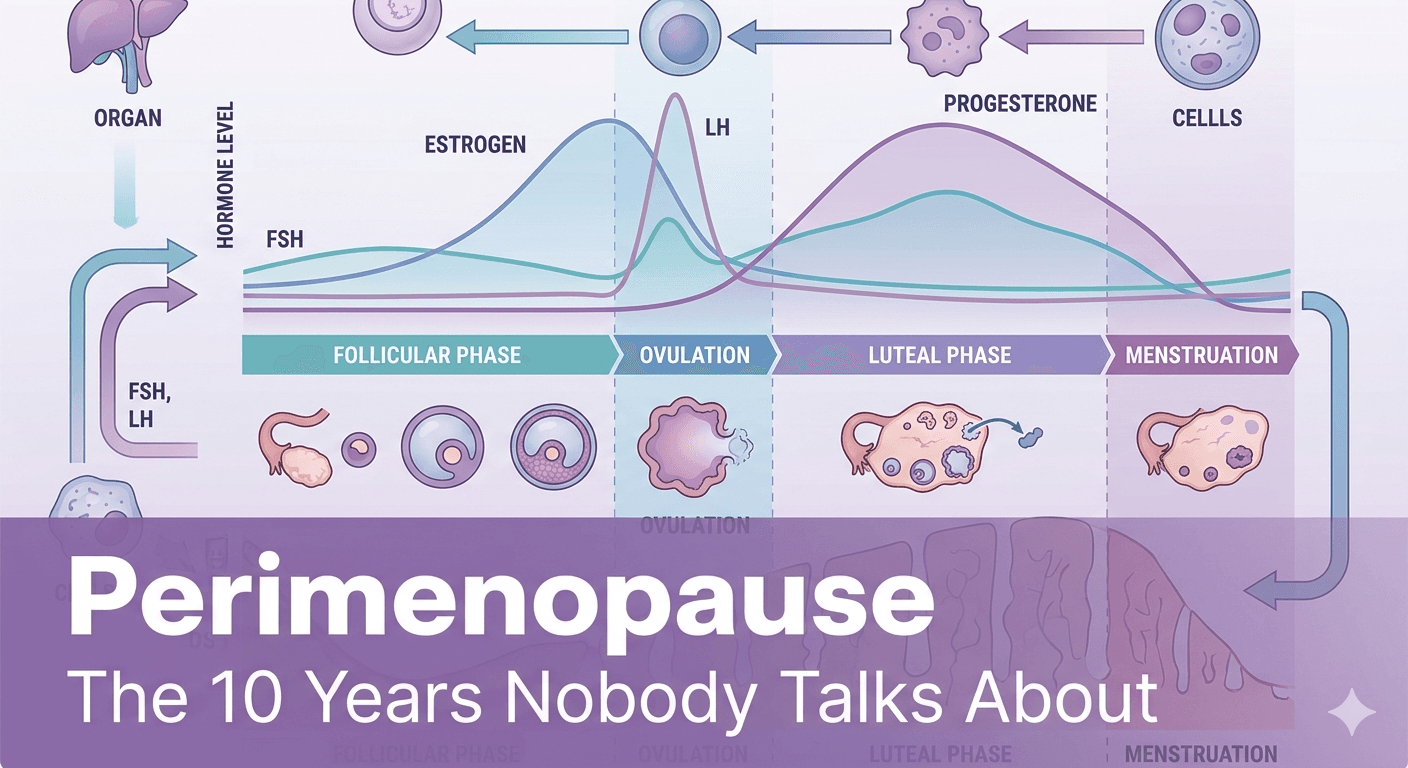
Your ovaries contain a fixed number of follicles from birth — each follicle capable of producing an egg and the hormones oestrogen and progesterone. From puberty onward, follicles are used with each menstrual cycle. As you approach your late 30s and 40s, the remaining follicles become less responsive to the hormonal signals (FSH and LH) from your brain that trigger ovulation.
The result is erratic hormonal production — particularly of oestrogen and progesterone — that fluctuates dramatically from month to month, week to week, and even day to day.
It is this hormonal volatility — not simply low oestrogen — that drives the symptoms of perimenopause. Oestrogen can actually be quite high during perimenopause, particularly in the early stages. What's happening is the loss of rhythmic, predictable hormonal cycling that your body has been calibrated to for decades.
Key hormonal changes:
- FSH (Follicle Stimulating Hormone) rises — your brain tries increasingly hard to stimulate less-responsive ovaries
- Oestrogen fluctuates wildly — can be very high one week and very low the next
- Progesterone declines — particularly in cycles where ovulation doesn't occur (anovulatory cycles)
- Testosterone declines — affecting libido, energy and motivation
- AMH (Anti-Mullerian Hormone) falls — a marker of remaining ovarian reserve that begins declining years before other symptoms appear
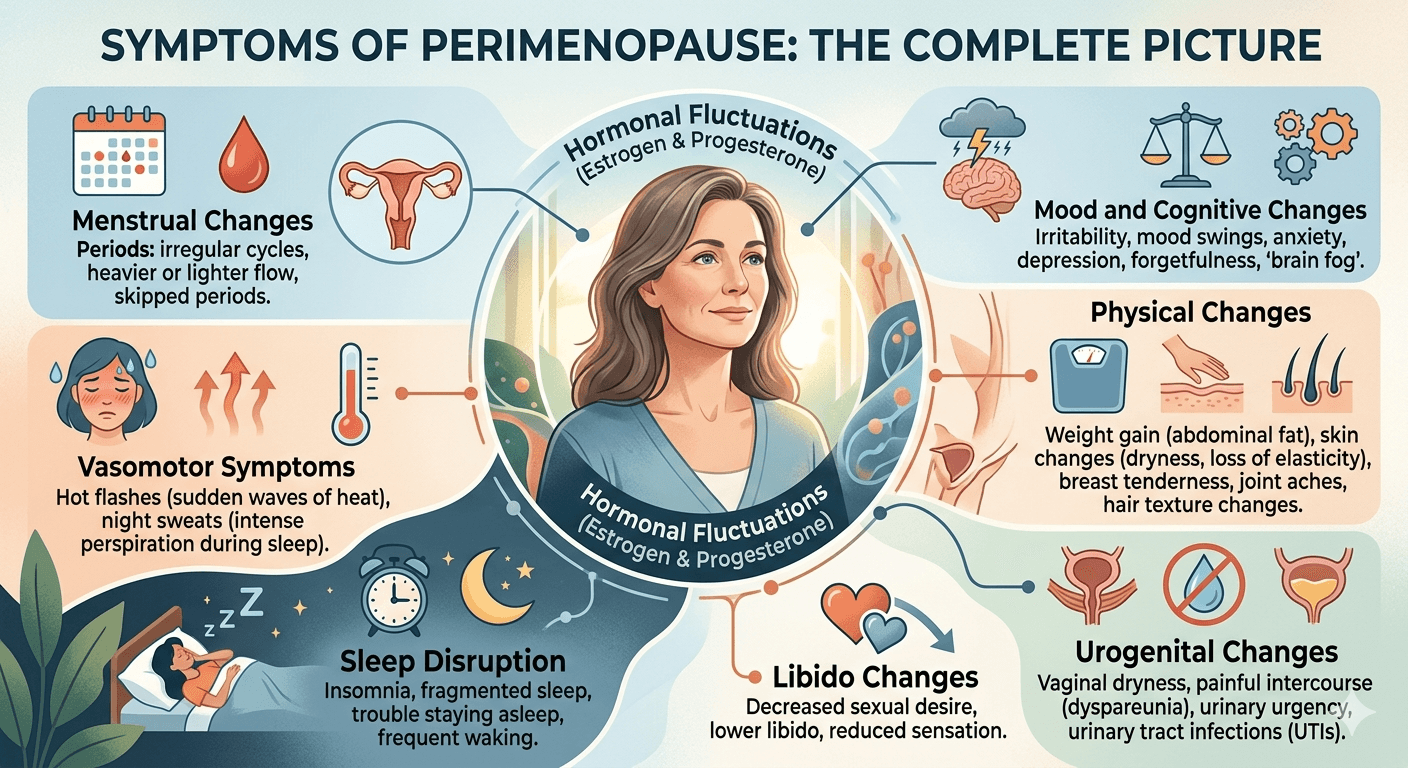
Symptoms of Perimenopause — The Complete Picture
This is where the information gap is most damaging. Most women associate menopause with hot flashes and periods stopping. But perimenopause has a much wider and more complex symptom picture — many of which are misattributed to stress, thyroid issues or depression.
Menstrual changes:
- Irregular cycle length — cycles may shorten (from 28 days to 21 days) before eventually lengthening
- Heavier than usual periods — often the first noticeable change
- Occasional missed periods
- Spotting between periods
- More intense PMS than previously experienced
Vasomotor symptoms:
- Hot flashes — sudden waves of heat, often starting in the chest and moving upward
- Night sweats — waking drenched in perspiration
- Palpitations — racing or irregular heartbeat, particularly during hot flashes
Sleep disruption:
- Difficulty falling asleep despite exhaustion
- Waking at 2-4am and unable to return to sleep
- Vivid, disturbing dreams
Mood and cognitive changes:
- Anxiety — particularly new-onset anxiety or worsening of existing anxiety
- Irritability that feels disproportionate to circumstances
- Low mood or depressive episodes
- Brain fog — difficulty concentrating, forgetting words, feeling mentally slow
- Loss of motivation and drive
Physical changes:
- Weight gain particularly around the abdomen — even without dietary changes
- Joint pain and stiffness — oestrogen has anti-inflammatory effects; its decline increases joint inflammation
- Hair thinning — both oestrogen and progesterone support hair growth
- Skin changes — dryness, loss of elasticity
- Breast tenderness — paradoxically, high oestrogen in early perimenopause can cause breast soreness
Urogenital changes:
- Vaginal dryness and discomfort
- Increased frequency of urinary tract infections
- Stress urinary incontinence — leaking with coughing, sneezing or exercise
Libido changes:
- Reduced sexual desire
- Reduced arousal and sensitivity
- Discomfort during intercourse due to vaginal changes
Why Indian Women Are Particularly Underserved
Perimenopause in India carries an additional burden that women in Western countries don't face to the same degree — cultural invisibility.
In Indian culture, menstruation is often treated as something private, even shameful. Menopause — and therefore perimenopause — receives even less acknowledgment. Many Indian women have no vocabulary for what they're experiencing. They don't discuss it with friends, don't raise it with doctors, and often interpret their symptoms as signs of serious illness, mental health crisis, or simply "getting old."
Healthcare access compounds this. Many Indian gynaecologists focus primarily on reproductive health — pregnancy, contraception, menstrual disorders — with less training and attention given to perimenopausal care. Women who raise symptoms are often told their blood tests are normal and sent home.
The emotional cost of this invisibility is enormous. Women in their prime — capable, accomplished, experienced — are struggling silently through a major biological transition while trying to maintain all their other roles without support or acknowledgment.
Diagnosis — Why It's Often Missed
Perimenopause is a clinical diagnosis — meaning it is primarily based on symptoms and age, not blood tests alone.
This is where many Indian women fall through the cracks. FSH levels — often the only test ordered — can appear normal in perimenopause because they fluctuate. A single blood test on a single day cannot capture the hormonal volatility of the perimenopausal transition.
If you are between 35-50 years old and experiencing multiple symptoms from the list above — particularly irregular periods, sleep disruption, mood changes and hot flashes — perimenopause should be on your differential diagnosis regardless of what your blood tests show.
Ask your gynaecologist specifically about perimenopause. Come prepared with a symptom diary — tracking your cycle patterns, sleep quality, mood and physical symptoms over 2-3 months gives far more diagnostic information than a blood test.
Management — What Actually Helps
Lifestyle interventions — the foundation:
Exercise is the single most powerful lifestyle intervention for perimenopausal symptoms. Specifically:
- Resistance training (weights, resistance bands) — crucial for maintaining muscle mass and bone density as oestrogen declines. Aim for 2-3 sessions per week
- Cardiovascular exercise — reduces hot flash frequency and severity, improves mood and sleep
- Yoga — particularly effective for mood, anxiety and sleep quality in perimenopause
Nutrition:
- Increase protein significantly — declining oestrogen xaccelerates muscle loss. Aim for 1.2-1.6g per kg body weight daily
- Calcium and Vitamin D — bone density begins declining in perimenopause. Ragi, sesame seeds, dairy and sunlight exposure are essential
- Reduce refined carbohydrates — insulin resistance worsens in perimenopause; blood sugar stability reduces hot flashes and mood swings
- Phytoestrogens — soy, flaxseeds, sesame seeds and chickpeas contain plant compounds that mildly mimic oestrogen and may reduce hot flash severity
Sleep hygiene:
- Consistent bedtime and wake time
- Keep bedroom cool — particularly important for night sweats
- Avoid alcohol — worsens night sweats significantly despite seeming to help initially
Stress management:
- Chronic stress dramatically worsens perimenopausal symptoms through cortisol-oestrogen interactions
- Pranayama, meditation and adequate rest are not luxuries during perimenopause — they are medicine
Medical Treatments — Knowing Your Options
Menopausal Hormone Therapy (MHT) — previously called HRT:
MHT involves supplementing declining hormones — oestrogen alone (for women without a uterus) or oestrogen combined with progesterone (for women with a uterus).
Modern MHT, when prescribed appropriately and started within 10 years of menopause, has a strong safety profile and is highly effective for:
- Hot flashes and night sweats
- Sleep disruption
- Mood symptoms
- Vaginal dryness
- Bone density preservation
The old fears about MHT — based on a 2002 study with methodological limitations — have been significantly revised. Current evidence, including the DIVA and NICE guidelines, supports that MHT is appropriate and beneficial for most healthy women in early perimenopause.
Speak to your gynaecologist about whether MHT is appropriate for you. Many Indian women who would benefit enormously from MHT are never offered it because their doctors don't raise it and they don't know to ask.
Non-hormonal prescription options:
For women who cannot or choose not to use MHT:
- SSRIs and SNRIs — shown to reduce hot flash frequency by 50-60%
- Gabapentin — effective for night sweats and sleep disruption
- Fezolinetant — a newer non-hormonal option targeting the brain pathways that trigger hot flashes
Vaginal oestrogen:
For urogenital symptoms specifically — vaginal dryness, discomfort, recurrent UTIs — localised vaginal oestrogen (cream, ring or tablet) is extremely safe and effective. The systemic absorption is minimal and it carries far fewer risks than systemic MHT.
The Conversation India Needs to Have
Perimenopause is not a disease. It is a natural biological transition — as natural as puberty. But like puberty, it requires information, support and sometimes medical assistance to navigate well.
Indian women deserve to approach this transition informed — not blindsided by symptoms they've never heard of, misdiagnosed with anxiety or thyroid disease, or dismissed with "everything looks normal."
If you are in your late 30s or 40s and recognising yourself in this blog — start tracking your symptoms. Talk to your gynaecologist specifically about perimenopause. Connect with other women going through the same transition.
You are not going crazy. You are not "just stressed." Your body is going through one of the most significant hormonal transitions of your life. And with the right information and support — you can navigate it with clarity, confidence and even grace.
🛒 Recommended Product
Sleep disruption is one of the most common and distressing symptoms of perimenopause. A good pregnancy and body pillow supports better sleeping positions during this transition — reducing the joint pain and discomfort that also commonly increases during perimenopause and helping you maintain the sleep quality your body needs for hormonal recovery.
View Pregnancy Support Pillow on Amazon →References
- Harlow SD, et al. Executive summary of STRAW+10. Menopause. 2012;19(4):387-395.
- Sharma S, Mahajan N. Perimenopausal symptoms in Indian women. J Midlife Health. 2015;6(2):77-83.
- Mishra GD, Kuh D. Health symptoms during midlife in relation to menopausal transition. BMJ. 2012;344:e402.
Written by — Dharmil Pandya
Medical Writer | Founder, Healthier Tomorrow
#PerimenopauseIndia #WomensHealth #HormonalHealth #IndianWomen #MenopauseAwareness